
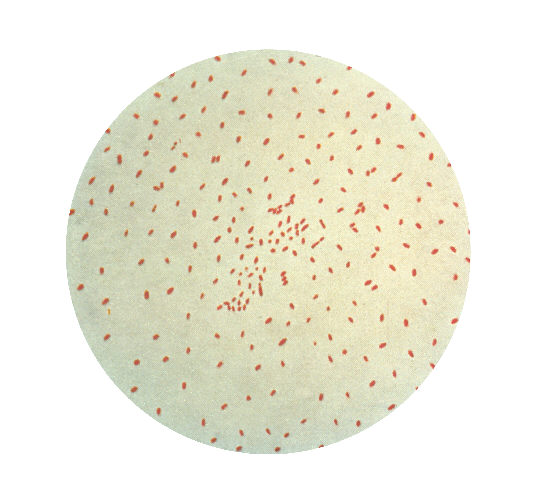
Bordetella pertussis (pictured below) is a gram negative, rod-shaped, obligate aerobe bacterium that causes pertussis, better known as whooping cough. Protection against this disease, which presents in three stages and is characterized by a “whooping” cough that persists for 4-8 weeks, is included in the DTaP vaccine for young children (0-6 years) and the TDaP vaccine for teens and adults. Four rounds of vaccination are administered prior to 18 months, once between the ages of 4-6, once between ages 11-12, and once during pregnancy (weeks 27-36). This sequence of vaccinations indicates a low strength immune response per injection. In 1997 the vaccine was altered from a form containing whole inactivated bacterial cells to DTaP which instead contains subunits (acelluar, aP vaccine) and is given in combination with tetanus and diphtheria boosters. The cellular vaccination produced an effective immune response, dramatically decreasing the incidence of pertussis, but had severe side effects. DTaP has no notable side effects but elicits a weaker immune response.
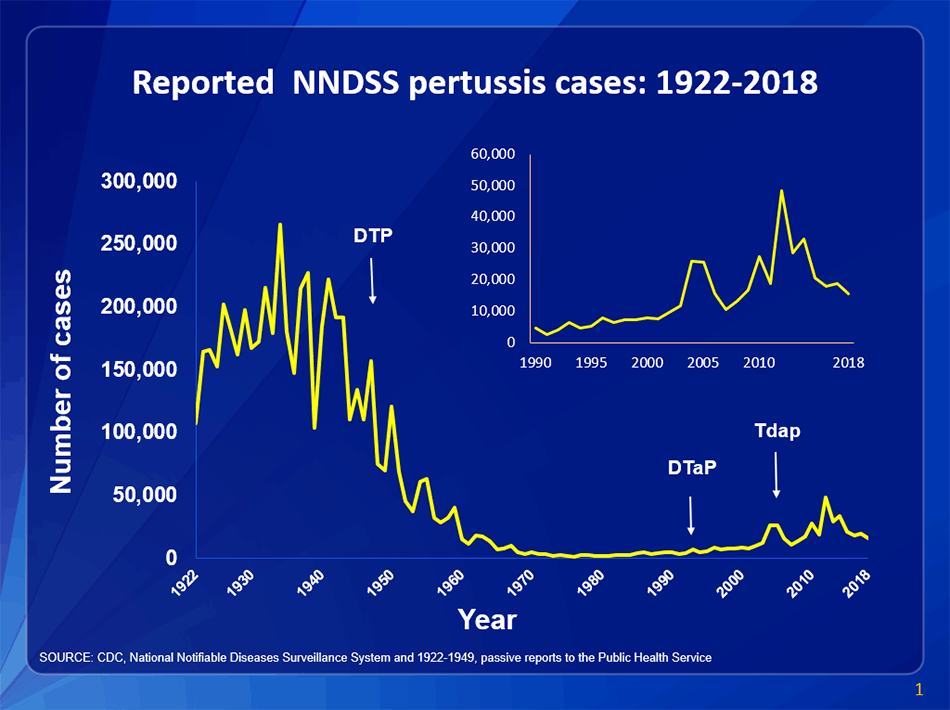
In recent years, the extent of waning immunity has been uncovered as outbreaks in fully vaccinated individuals continue to occur, in increasing amounts since the aP vaccine’s introduction (view trends). My younger sister, fully vaccinated, contracted the disease in 2015 during middle school. It was transmitted via respiratory droplets, with less severe presentation, to our cousin of the same age. My sisters progression aligned precisely with the 3 characteristic stages: catarrhal stage (1-2 weeks of typical upper respiratory symptoms, with low fever), paroxysmal stage (2-4 weeks of a violent whooping cough inducing vomiting and difficulty breathing), and convalescent stage (recovery with coughing attacks gradually decreasing). It seemed impossible, that after 6 vaccinations, the disease could present so severely in a young healthy individual. The danger for newborns and immunocompromised individuals can be thus inferred. Additionally, it was interesting that the bacterium was only transmitted to one other family member who was on the exact same vaccination timeline. My grandfather (a pediatrician), and my father (an internal medicine doctor), suspected that the pre-teen booster they both received conferred lower immunity in comparison to boosters of other years. These instances observed in my family correlate with the spike (above graph) between 2010 and 2018.
Besides the inherent weakness in the vaccine containing antigen rather than whole cells, there is also some evidence that B. pertussis has undergone vaccine induced selection. Researchers are searching for alternative forms to the aP, that might prevent waning immunity and outbreaks. The live attenuated BPZE1 intranasal vaccine is currently undergoing trials. This form is noted to prevent nasal colonization of B. pertussis, reducing transmission and potentially disease incidence. Limited side effects were noted in the preliminary human experiments (results posted January 2, 2020). The DTaP and TDaP vaccines still significantly reduce disease risk for pertussis when unvaccinated, partially vaccinated, and fully vaccinated individuals are compared. However, there is always room for improvement. Reducing the ability of transmission via the nasal route would positively inhibit the disease threats to infants <1, to whom the disease is most fatal.
